Metro Colon Rectum - Proctology Corner – Fissure
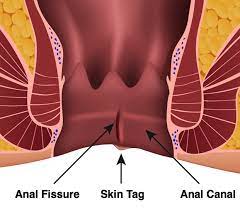
Anal fissures are one of the most painful conditions patients suffer from. An anal fissure is a tear in the lining of the anal canal that exposes the internal sphincter muscle. The most important part of managing anal fissures is symptom control through soft stools and internal sphincter muscle relaxation. Our practice has a step-up treatment algorithm that is both conservative and effective.
Fissures are caused by hard stools or dilation of the anal canal that leads to the primary tear. Once the tear occurs, the internal sphincter muscle spasms and decreases blood flow to the area. This causes pain and prevents fast healing. The pain leads to fear of defecating and constipation which leads to harder stools. As you can imagine, these symptoms can spiral out of control.
The management of fissures focuses on keeping stool soft and relaxing the internal sphincter muscle and starts in the office. Stool softening agents like fiber, colace, and miralax can be helpful. Avoiding straining or pushing can also help. Prescription medications provided by our practice will involve a muscle relaxer and a local anesthetic. The ointment we use is 0.5% nifedipine (a smooth muscle relaxer) mixed with 5.0% lidocaine (a local anesthetic). The ointment is applied twice daily and after bowel movements. A course of nifedipine/lidocaine can last for 2-3 months and is considered office-based treatment.
When patients do not have an adequate response to office-based treatments, we progress to a targeted injection of botulinum toxin (Botox) into the internal sphincter muscle. The botox lasts for three months and chemically de-innervates the muscle preventing it from spasming and causing pain. Botox does not treat the fissure, it improves healing by increasing blood supply by decreasing muscle spasm and decreases pain through decreasing spasm. During the procedure to inject the botox, our practice may debride the fissure or destroy it while you are asleep to help healing.
When patients do not have an adequate response to a botox injection and office-based treatments, our practice may offer a tailored sphincterotomy. This is a permanent cutting of the internal sphincter that mechanically breaks the muscle spasm. This is one of the final stages of treatment of chronic anal fissures. Most patients do not require the sphincterotomy to treat their anal fissure.
The main risk of the treatments for anal fissures is fecal incontinence. While true fecal incontinence is rare, some patients experience a weakening of their sphincter muscle and a sense of urgency when defecating. This is usually temporary and our practice has treatments to help minimize life-style limitations.