Metro Colon Rectum - Proctology Corner – Fistula
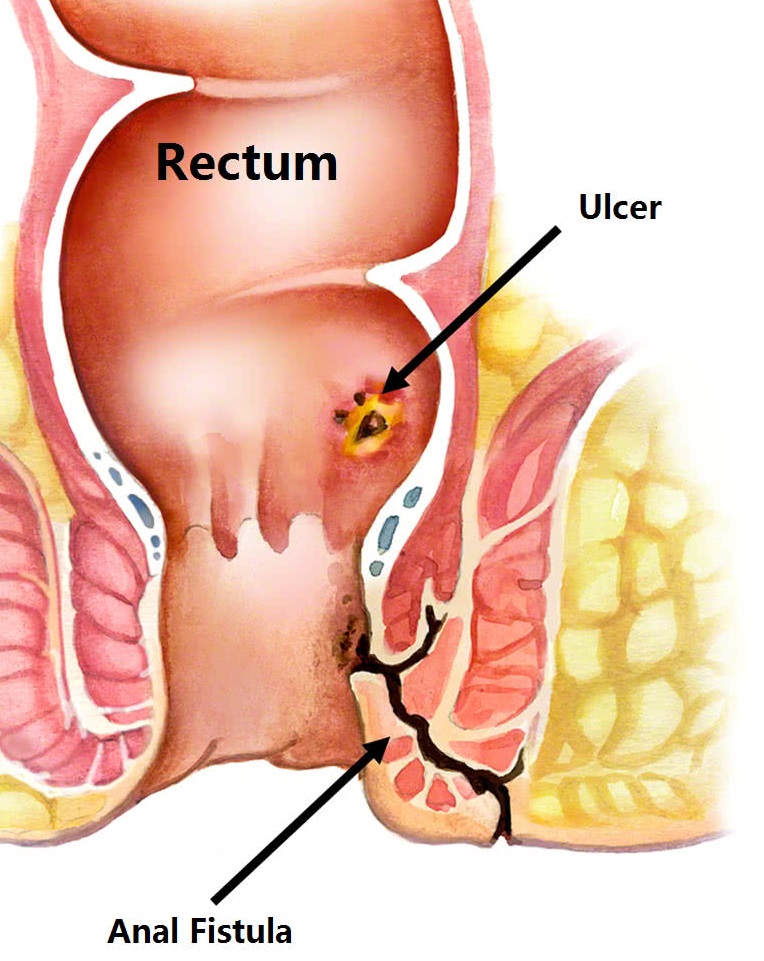
Fistulas are connections starting from one space or organ to another. Anorectal fistulas are connections between the anus or rectum and the perianal skin. The most important part of managing fistulas is what is encompassed within the fistula tract. Fistulas usually develop from trapped infection or chronic inflammation such as an anorectal abscess. The most common type of fistula is the anal-cutaneous fistula or fistula-in-ano.
The management of fistulas focuses on first removing the source of the infection or inflammation. Once the fistula is “controlled” the next step is to let the body heal. This usually takes two to three months and corresponds with the body’s healing process at a cellular level. The final step is to close the fistula. This entire process can take multiple months and requires more than one surgery even if everything goes perfectly.
The most important aspect of the surgical management of anal fistulas is accurately determining the extent of the fistula and the size of the sphincter complex. The sphincter complex is made up of two muscles, the internal sphincter, and the external sphincter. The internal sphincter provides a subconscious level of fecal continence, and the external sphincter provides a conscious level of continence. Simply stated, the external sphincter helps us make it to the bathroom after a spicy meal while the internal sphincter helps us not poop our pants while having a polite conversation.
For fistulas that encompass less than 20% of the sphincter complex, cutting of the fistula tract is usually curative. For fistulas that encompass more than 20% of the sphincter complex, cutting the fistula is curative but has a high risk of sphincter failure. When more than 20% of the sphincter complex is involved or sphincter failure is a concern, a seton is instead placed to stage the fistula. A seton is a benign flexible rubber. The seton provides a path of least resistance for the drainage of infectious or inflammatory materials and stays in place for two to three months.
Once the body has healed, a second procedure is required to close the fistula. If less than 20% of the sphincter complex is involved a fistulotomy is sufficient. However, if more than 20% of the sphincter is involved a complex fistula closure is required. Two complex fistula closure procedures are the Ligation of Intersphincteric Fistula Tract (LIFT) or an Endo-Rectal Advancement Flap (ERAF). The success rate of these complex fistula closure procedures is around 75%. Both complex closures require a full bowel preparation to decrease the risk of disruption and neither interrupt sphincter function.